For the urine to exit the bladder, both the autonomically controlled internal sphincter and the voluntarily controlled external sphincter must be opened. Problems with these muscles can lead to incontinence.
The urinary bladder usually holds 300-350 ml of urine. As urine accumulates, the rugae flatten and the wall of the bladder thins as it stretches, allowing the bladder to store larger amounts of urine without a significant rise in internal pressure.
 |
| bladder picture |
The urinary bladder is a muscular sac
in the pelvis, just above and behind the pubic bone. When empty, the
bladder is about the size and shape of a pear.
 |
The internal sphincter is a continuation of the detrusor muscle and is made of smooth muscle, therefore it is under involuntary or autonomic control. This is the primary muscle for prohibiting the release of urine.
The external sphincter muscle of urethra in males is a secondary sphincter to control the flow of urine through
the urethra. Unlike the internal sphincter muscle, the external
sphincter is made of skeletal muscle, therefore it is under voluntary control of the somatic nervous system.
share courtesy: wikipedia.org
|
Urine is made in
the kidneys, and travels down two tubes called ureters to the bladder.
The bladder stores urine, allowing urination to be infrequent and
voluntary. The bladder is lined by layers of muscle tissue that stretch
to accommodate urine. The normal capacity of the bladder is 400 to 600
mL.
During urination, the bladder muscles contract, and two
sphincters (valves) open to allow urine to flow out. Urine exits the
bladder into the urethra, which carries urine out of the body. Because
it passes through the penis, the urethra is longer in men (8 inches)
than in women (1.5 inches).
Urinary retention:
Urine does not exit the bladder normally due to obstruction or
suppressed bladder muscle activity. The bladder may swell to hold more
than a quart of urine.
Causes of Urinary retention: There are two general types of urinary
retention: obstructive and non-obstructive. If there is an obstruction
(for example, kidney stones), urine cannot flow freely through the
urinary track. Non-obstructive causes include a weak bladder muscle and
nerve problems that interfere with signals between the brain and the
bladder. If the nerves aren’t working properly, the brain may not get
the message that the bladder is full.
Some of the most common causes of non-obstructive urinary retention are:
- Stroke
- Vaginal childbirth
- Pelvic injury or trauma
- Impaired muscle or nerve function due to medication or anesthesia
- Accidents that injure the brain or spinal cord
Obstructive retention may result from:
- Cancer
- Kidney or bladder stones
- Enlarged prostate (BPH) in men
In acute urine retention, but the person is unable to pass the urine, resulting in significant pain.
Chronic urine retention is where a person is able to pass small quantities of urine with difficulty and the bladder never completely empties. It is usually painless. Symptoms of acute urine retention include lower abdominal pain, a sensation of fullness in the lower abdomen, and a painful urge and inability to pass urine. Chronic urine retention symptoms include swelling of the abdomen, a frequent need to urinate, difficulty in starting the urine flow, a weak urine flow, and dribbling at the end of urinating and between urinating. Treatment options include temporary or permanent catheterization, medication, treating the underlying cause, herbal therapies, and homoeopathy.
Acute urinary retention (AUR) is the sudden inability to pass urine. It is usually painful and requires emergency treatment with a urinary catheter.
Causes: These are numerous and can be classified as:
- In men - benign prostatic hypertrophy (BPH), meatal stenosis, paraphimosis, penile constricting bands, phimosis, prostate cancer.
- In women - prolapse (cystocele, rectocele, uterine), pelvic mass (gynaecological malignancy, uterine fibroid, ovarian cyst), retroverted gravid uterus.
- In both - bladder calculi, bladder cancer, faecal impaction, gastrointestinal or retroperitoneal malignancy, urethral strictures, foreign bodies, stones.
Infectious and inflammatory:
- In men - balanitis, prostatitis and prostatic abscess.
- In women - acute vulvovaginitis, vaginal lichen planus and lichen sclerosis, vaginal pemphigus.
- In both - bilharzia, cystitis, herpes simplex virus (particularly primary infection), peri-urethral abscess, varicella-zoster virus.
 |
| A healthy human prostate is classically said to be slightly larger than a walnut. The mean weight of the "normal" prostate in adult males is about 11 grams, usually ranging between 7 and 16 grams. It surrounds the urethra just below the urinary bladder and can be felt during a rectal exam. It is the only exocrine organ located in the midline in humans and similar animals. share courtesy: wikipedia.org |
#BPH is by far the most common cause of urinary retention. Alpha-1 blockers given before catheter removal increase the chances of a successful TWOC.
 |
| Diagram illustrating normal prostate (left) and benign prostatic hyperplasia (right). share courtesy: http://en.wikipedia.org |
Benign Prostatic Hyperplasia: BPH involves hyperplasia of prostatic stromal and epithelial
cells, resulting in the formation of large, fairly discrete nodules in
the periurethral region of the prostate. When sufficiently large, the
nodules compress the urethral canal to cause partial, or sometimes virtually complete, obstruction of the urethra, which interferes with the normal flow of urine. It leads to symptoms of urinary hesitancy, frequent urination, dysuria (painful urination), increased risk of urinary tract infections, and urinary retention. Although prostate specific antigen levels may be elevated in these patients because of increased organ volume and inflammation due to urinary tract infections, BPH does not lead to cancer or increase the risk of cancer.
BPH involves hyperplasia (an increase in the number of cells) rather than hypertrophy (a growth in the size of individual cells), but the two terms are often used interchangeably, even amongst urologists.  |
| Its prevalence is age dependent. Histological evidence of BPH is rarely observed in men under 50 years of age, but by age 80 virtually all men will have some histological evidence of the process. It is unclear what specific factors regulate the degree of hyperplasia, which ultimately dictates the size of the prostate gland, nor is there any consensus regarding the prostate size that qualifies for the diagnosis of benign prostatic enlargement (BPE). |
Alpha blockers for the treatment of Benign Prostatic Hyperplasia:
The
relative degree of stromal and epithelial hyperplasia is highly
variable. Overall, approximately 80% and 20% of the hyperplastic volume
is composed of stromal and epithelial elements, respectively. Half of the stromal hyperplasia is composed of smooth-muscle elements. For decades, it was assumed that the enlarged hyperplastic prostate caused BOO via both dynamic and static mechanisms. The dynamic obstruction was thought to be the result of smooth-muscle
hyperplasia causing a functional obstruction and static obstruction
arising from the bulk enlargement of the hyperplastic process
encroaching upon the prostatic urethra.Marco Caine demonstrated in 1975 that strips of human prostate contracted in response to norepinephrine.The norepinephrine-induced contractions were inhibited by pretreatment with phenoxybenzamine, a non-selective inhibitor of alpha adrenoceptor. These studies implicated the alpha adrenoceptor as the mediator of prostate smooth-muscle contraction. Lepor and Shapiro were the first investigators to characterize both alpha 1 and 2 adrenoceptors in the human prostate using radioligand binding studies.
Tamsulosin was the third alpha 1
blocker to be approved for the treatment of BPH. Tamsulosin was brought
to market as the first subtype selective alpha 1 antagonist for the
treatment of BPH. Tamsulosin alpha 1 subtype selective was supported by
binding studies, which showed that tamsulosin was approximately tenfold
more selective for the alpha 1a versus alpha 1b subtype.
There was no demonstrable subtype selectivity of tamsulosin for the
alpha 1a versus alpha 1d subtypes. The modest receptor selectivity of
tamsulosin is not sufficient to result in a clinically meaningful
advantage. Typically, clinical advantages attributed to pharmacological
selectivity require a receptor selectivity well beyond the tenfold
difference observed with tamsulosin.
Two pivotal trials of tamsulosin supported the NDA for the treatment of symptomatic BPH. Both 0.4 and 0.8 mg of tamsulosin achieved clinically significant improvements in symptom scores and peak flow rate.
The ability of the 0.4 mg tamsulosin dose to achieve a clinically
significant effect without the requirement for dose titration
represented a unique advantage over the other approved alpha blockers.
Although a 0.8 mg daily dose was more effective than 0.4 mg, it did not
gain popularity because it required both dose titration and taking 2
tablets of 0.4 mg. (A 0.8 mg tablet was not commercially available.) The
primary reason tamsulosin was prescribed over terazosin and doxazosin
was not due to greater efficacy or better tolerability, but simply the
lack of dose titration. The prescribing community placed a greater value
on eliminating the dose response at the expense of increasing the
incidence of ejaculatory dysfunction, which was thought to be retrograde
ejaculation as a result of relaxation of the bladder neck. Recent
studies have demonstrated that tamsulosin causes anejaculation rather
than retrograde ejaculation.
The mechanism for the increased incidence of ejaculatory dysfunction
associated with tamsulosin has been attributed to its affinity for
dopaminergic and other central nervous system receptors.
 |
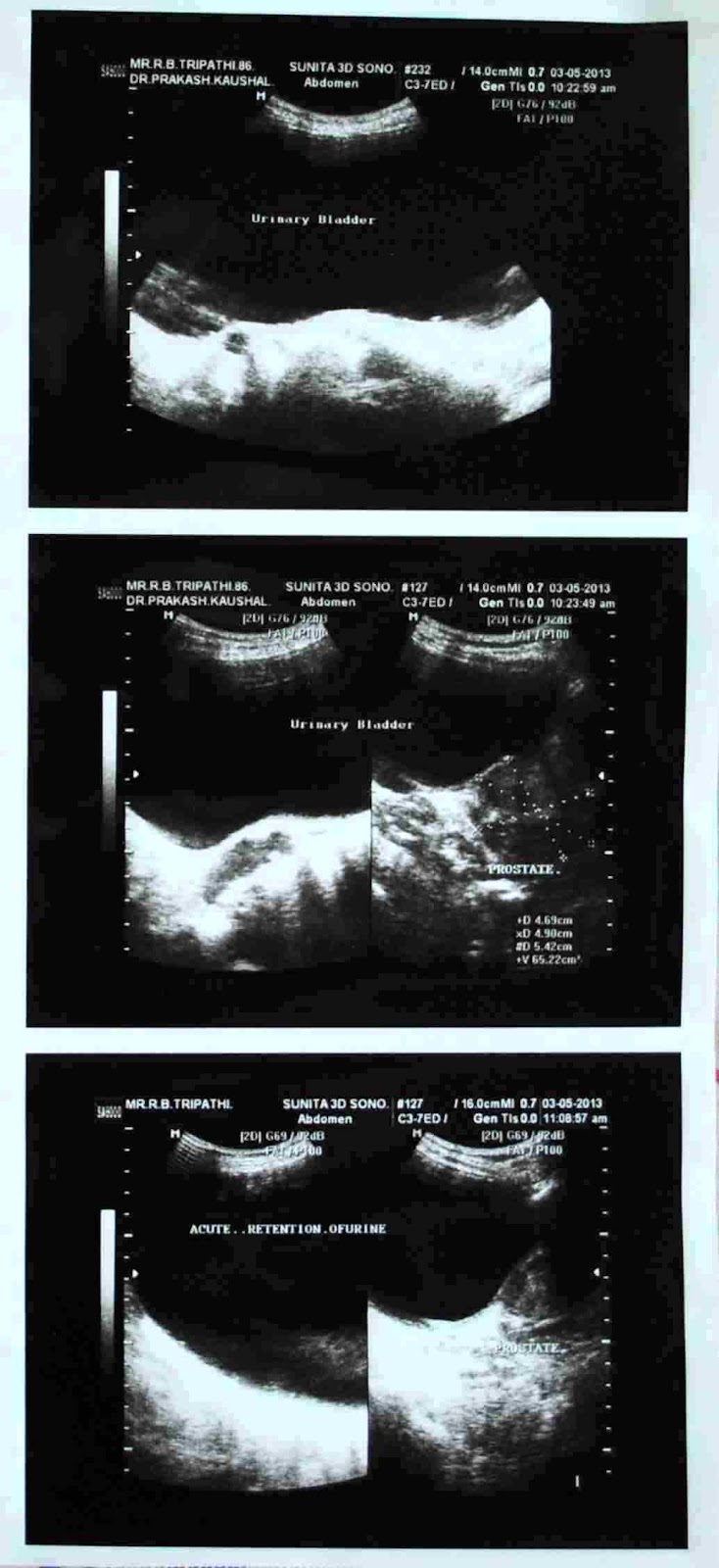
A case report:
Age: 86 years male, Acute urinary retention 1400 ml,
Prostate enlarge, 65 gm in weight,
Chronic retention of urine
cause may be BPH with
#As seen in above sonograph Bladder Neck Obstruction.
picture
|
An
episode of acute urinary retention is no longer an absolute indication
for surgical intervention. Alpha blockers are a very reasonable initial
option for managing acute urinary retention.
Following sites referred thankfully and reference for further detail:
http://en.wikipedia.org
http://www.webmd.com
http://www.medtronic.com
http://www.naturaltherapypages.com.au/glossary/Urine_Retention#ixzz2T2pDuWCp
http://www.patient.co.uk/doctor/acute-urinary-retention
NCBI journal Rev Urol. 2007 Fall; 9(4): 181–190
file:///E:/Alpha%20Blockers%20for%20the%20Treatment%20of%20Benign%20Prostatic%20Hyperplasia.htm
Some abbreviations used:
Food and Drug Administration (FDA)
lower urinary tract symptoms (LUTS)
bladder outlet obstruction (BOO)
benign prostatic enlargement (BPE)
benign prostatic hyperplasia (BPH)
Medical Therapy of Prostatatic Symptoms (MTOPS)
The American Urological Association
Symptoms Index (AUASI)
International Prostate Symptom Index
Score (IPSS)
new drug application (NDA)
Three
subtypes of the alpha 1 adrenoceptor (alpha 1a, alpha 1b, alpha 1d)
have been cloned and pharmacologically characterized.
The Antihypertensive
and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT)